Light Timing for Better Sleep: Morning Sun, Evening Dark, and Where Red Light Fits
How light timing shapes sleep: get bright light in the morning, dim it at night, and see what the evidence actually says about red light therapy and melatonin.

Answer first: The single most reliable way to use light for better sleep is timing, not gadgets — bright light in the morning, dim and warm light at night. That pattern keeps your internal clock and your melatonin on a healthy schedule. Red and near-infrared light therapy is interesting here for one specific reason: unlike bright blue-white light, it appears far less likely to suppress melatonin, so it is a gentle choice for the evening. But the direct evidence that red light improves sleep is still limited and early, and you should treat it as a supporting habit, not a cure.
This article separates two things that often get blurred together: (a) the well-established science of how light timing and brightness set your body clock, and (b) the much smaller, emerging body of research on whether red/near-infrared light therapy (photobiomodulation, or PBM) specifically helps sleep. Keeping those separate is the difference between honest guidance and marketing.
How light sets your body clock
Almost every cell in your body runs on a roughly 24-hour cycle. The master conductor is your circadian rhythm — an internal clock, housed in a small cluster of brain cells called the suprachiasmatic nucleus, that coordinates when you feel sleepy, when your body temperature dips, and when hormones rise and fall. Left alone in constant darkness, this clock runs close to, but not exactly, 24 hours, so it needs a daily “reset” signal to stay aligned with the outside world.
That reset signal is light reaching the eye. Specialized cells in the retina — distinct from the rods and cones you use to see — contain a pigment called melanopsin and act as dedicated brightness detectors. They are most sensitive to shorter, blue-rich wavelengths (around 480 nm), and they send that “how bright is it?” information straight to the clock. As a comprehensive review in Somnologie describes, this light pathway is the primary way the body synchronizes its internal rhythms to the 24-hour solar day (Blume et al., 2019).
This is the crucial idea behind everything that follows: light is not just illumination, it is information. The same light that lets you read a book is also telling your brain what time it is. When the timing of that signal matches the real day — bright when the sun is up, dark when it is down — your clock stays anchored and your sleep tends to come easily at a consistent time. When the signal is scrambled — dim, gray indoor days and bright, screen-lit nights — the clock drifts, and sleep timing and quality drift with it.
What “circadian misalignment” feels like
When your internal clock and your actual schedule disagree, the result is circadian misalignment. You have probably felt it as jet lag, or as the Monday-morning grogginess after a weekend of late nights (“social jet lag”). The common thread is that your body is being asked to sleep when its clock still thinks it is daytime, or to wake when its clock still says night. Fixing the light signal is the most direct way to bring the two back into agreement.
Two key terms: melatonin and lux
Melatonin is the hormone your brain releases in the evening as darkness approaches. It does not knock you out like a sedative; instead it is a signal — a chemical message that says “it is night, prepare for sleep.” Light, particularly bright or blue-rich light, suppresses melatonin. That is why evening light matters so much.
Lux is a measure of how much visible light reaches a surface (here, your eyes), weighted for how the human eye perceives brightness; irradiance is the related physics term for raw light energy per unit area (watts per square meter), which is what matters when we talk about wavelengths the eye barely registers, like near-infrared. The two are related but not identical, and the distinction becomes important later when we discuss red and near-infrared therapy, whose biological effects are described in irradiance rather than lux.
The everyday numbers are deeply unintuitive, because human eyes adapt so well that a dim room and bright daylight feel closer in brightness than they are:
- Candlelight / very dim room: under 10 lux
- Typical living room in the evening: ~100–300 lux
- Well-lit office: ~300–500 lux
- Overcast daylight outdoors: ~1,000–10,000 lux
- Direct summer sun: 50,000–100,000+ lux
The gap between “bright indoor room” and “dull cloudy day outside” can be a factor of ten or more. Your clock cares about these large differences far more than about which specific lamp you choose. This is exactly why “I get plenty of light indoors” is usually false from your body clock’s point of view: indoor light is often an order of magnitude too dim to act as a strong morning signal, and at the same time bright enough in the evening to act as a melatonin-suppressing one.
The clearest demonstration of how powerfully natural light sets the clock comes from a camping study: after a week outdoors with only sunlight and campfires, participants’ internal clocks shifted earlier and aligned tightly with sunrise and sunset, reversing the delay caused by modern indoor electric lighting (Wright et al., 2013).
Morning light: the most important signal
If you change one thing, make it morning light. Bright light early in the day does two useful things at once: it advances your clock (nudging your natural sleep time earlier) and it raises daytime alertness while reinforcing the day–night contrast your brain uses to time melatonin.
Why does morning light specifically advance the clock? Because the clock responds to light differently depending on when it arrives. Light in the morning (after your body’s lowest temperature point, which is usually a couple of hours before you wake) shifts the clock earlier; light in the late evening and at night shifts it later. This timing-dependent response is what chronobiologists call the phase-response curve. The practical upshot is intuitive once you know it: morning light helps you fall asleep and wake earlier, while evening light does the opposite.
Real-world data backs this up. A case-control study of office workers found that those seated near windows with greater daylight exposure slept about 46 minutes longer and reported better sleep quality on the Pittsburgh Sleep Quality Index than colleagues in windowless spaces (Boubekri et al., 2014). A field study using portable sleep monitoring (polysomnography) similarly linked earlier, brighter daytime light exposure to more slow-wave (deep) sleep that night (Wams et al., 2017). And the camping study mentioned earlier showed the effect at its most dramatic: a week of nothing but natural light shifted the entire group’s clocks earlier and tightened them to the solar day, with the biggest shifts in the people who had been the most “night-owl” beforehand (Wright et al., 2013).
How to get morning light
- Go outside within 1–2 hours of waking. Aim for 10–30 minutes. Even an overcast morning delivers far more light than your brightest indoor room.
- You do not need to look at the sun. Ambient daylight reaching your open eyes is enough — and staring at the sun is unsafe.
- Pair it with a routine — a walk, coffee on the porch, your commute on foot — so it actually happens daily.
- If you cannot get outside, sit near a bright window, or consider a clinician-recommended light box (commonly ~10,000 lux) used as directed, especially in winter.
Consistency matters more than perfection. The clock responds to a repeated daily pattern, so similar wake and light-exposure times every day — including weekends — produce the steadiest results. A single missed morning will not undo your progress, but a regular habit is what holds the clock in place over weeks. If you tend toward being a night owl and want to shift earlier, the combination of earlier morning light plus dimmer evenings is far more powerful than either change alone, because you are pushing the clock in the same direction from both ends of the day.
Evening light and melatonin: the part most people get wrong
In the evening, the goal flips: you want less light, and warmer, dimmer light. This is where modern life works against us, because bright indoor lighting and screens deliver exactly the kind of light that delays the clock and suppresses melatonin.
How big is the effect? In a tightly controlled study, exposure to ordinary room light before bedtime suppressed melatonin and shortened its nightly duration by roughly 90 minutes compared with dim light; light during the usual sleeping hours suppressed melatonin by more than 50% in most people (Gooley et al., 2011). Screens add to this: in a crossover trial, reading on a light-emitting e-reader before bed suppressed evening melatonin, delayed the circadian clock, lengthened the time to fall asleep, and reduced next-morning alertness compared with reading a printed book (Chang et al., 2015).
A broad systematic review of 128 studies reached the same conclusion: mistimed evening and night light disrupts circadian rhythm, with the strongest melatonin suppression at short (blue/violet) wavelengths (Tähkämö et al., 2019). The same review noted that sensitivity to evening light varies between people and tends to decline with age, so two people in the same brightly lit kitchen at night may have meaningfully different melatonin responses — which is one reason general “screen time” rules feel hit-or-miss.
It is worth being precise about what the evening problem actually is. The issue is not screens as objects, or even “blue light” as a villain in isolation — it is bright, blue-rich light delivered during the hours when melatonin should be rising. A dim phone at low brightness in warm mode is a far smaller signal than a brightly lit room with overhead LEDs. That reframing matters because it points to a realistic fix (dim and warm everything in the evening) rather than an unrealistic one (eliminate all screens forever).
Practical evening light hygiene
- Dim the house in the last 2–3 hours before bed; use lamps instead of bright overhead lights.
- Favor warm, low-color-temperature bulbs in the evening, and turn brightness down.
- Reduce screen brightness, enable night/warm modes, and ideally stop screens 30–60 minutes before sleep.
- Keep the bedroom dark overnight — blackout curtains or an eye mask help.
You do not need perfect darkness all evening; you need to avoid bright, blue-rich light during the window when melatonin should be climbing.
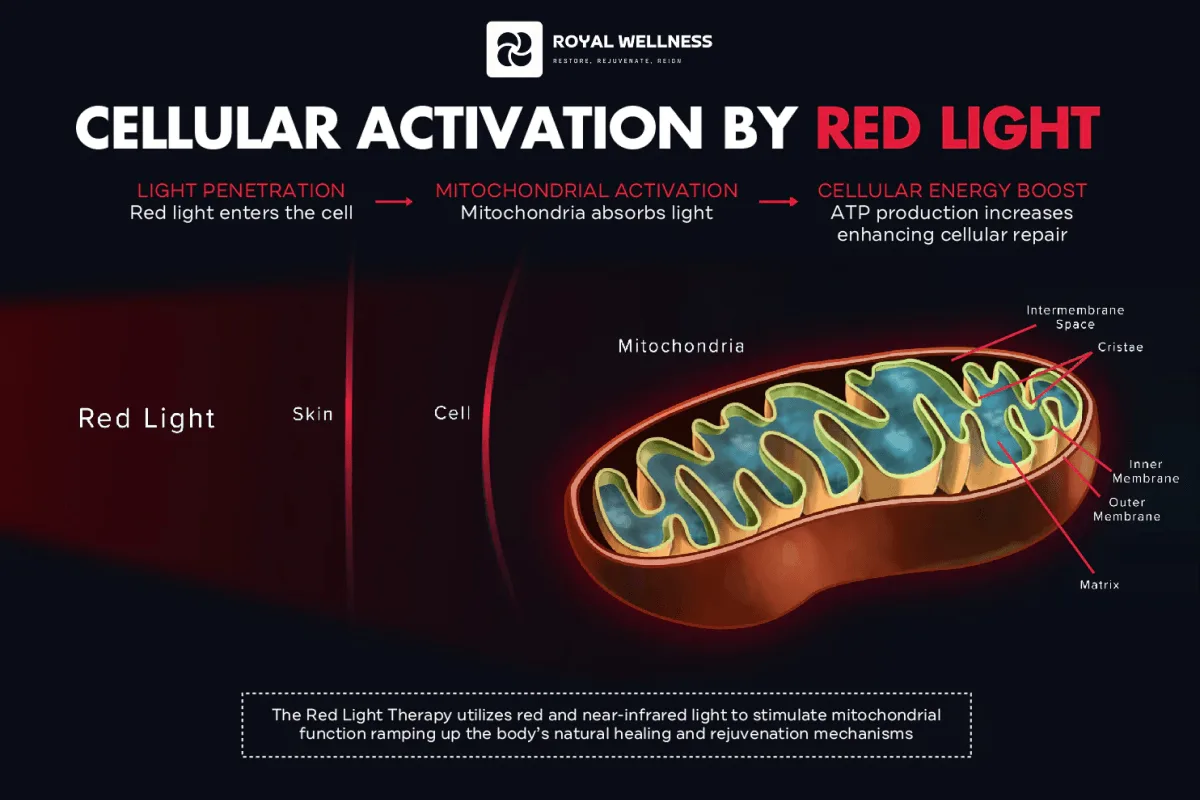
Where red and near-infrared light fit — and what the studies really show
Now to the topic many readers came for. Red light therapy (and near-infrared, together called photobiomodulation) uses specific longer wavelengths — typically red around 630–660 nm and near-infrared around 810–850 nm — delivered by LED panels or masks. It is studied mostly for skin, recovery, and pain. Its connection to sleep is more indirect, and the evidence is honestly thin. Two distinct claims need separating.
Claim 1: Red light is gentler on melatonin (better supported)
Because melatonin suppression is driven mainly by short, blue wavelengths, longer red wavelengths are far less disruptive to the circadian system. In one study, saturated red light delivered at low levels through closed eyelids did not suppress melatonin, which is why researchers explored it for reducing morning grogginess without throwing off the clock (Figueiro et al., 2019). The practical implication is modest but real: a warm, red-leaning, dim evening environment is circadian-friendly. That is about not harming melatonin — not about red light boosting sleep.
Claim 2: Red light therapy improves sleep (limited and emerging)
The single most-cited study here is small. Over 14 days, 20 elite female basketball players received nightly whole-body red-light treatment (658 nm). The treated group showed improved Pittsburgh Sleep Quality Index scores and higher serum melatonin than controls (Zhao et al., 2012). It is a genuinely interesting result — but it is one small trial, in a specific athletic population, with a placebo group of 20 total participants. It is a hypothesis-generating signal, not evidence that red light reliably improves sleep in the general public.
Why we are cautious — and why that is the right call
It would be easy for a company that sells red light devices to overstate this. We will not. Here is why the caution is appropriate rather than just conservative:
- Small samples. The athlete trial had 20 participants total. Small studies can show large effects by chance, and they need replication in bigger, more varied groups before we can generalize.
- Specific populations. Elite athletes recovering from heavy training are not the same as a desk worker with stress-related insomnia. What helps one group may not transfer.
- Mechanism is mostly indirect. The clearest, best-supported role for red light in sleep is what it doesn’t do — it doesn’t hammer melatonin the way blue-white light does. That is a reason it is compatible with good sleep hygiene, not evidence that it causes better sleep.
- Publication and commercial bias. Sleep is a heavily marketed category. Independent, well-controlled trials matter more here than glossy claims, and there simply are not many of them yet for red light and sleep.
Honest bottom line: there is not yet large, replicated, high-quality evidence that red or near-infrared light therapy directly improves sleep quality or insomnia for most people. The stronger, well-replicated lever for sleep is light timing and brightness — bright mornings, dim evenings. If you enjoy a red-light device, the most defensible sleep-related role is using it as a warm, melatonin-sparing part of an earlier wind-down — not as a treatment claim. You can read how we evaluate the literature on the science page, and browse the underlying papers in our research library.
A practical daily light-timing schedule
Use this as a flexible template, not a rigid prescription. The principle is simple: maximize bright light early, minimize bright/blue light late.
| Time of day | What to do with light |
|---|---|
| On waking | Open curtains immediately; get outside within 1–2 hours for 10–30 min of daylight |
| Mid-morning | Keep work areas bright; sit near a window if you can |
| Afternoon | Take a short outdoor break; let daytime stay bright and active |
| Early evening | Begin dimming overhead lights; switch to warm lamps; lower screen brightness |
| 2–3 hrs before bed | Keep lights low and warm; if using a red/NIR device, do it now, not at lights-out |
| 30–60 min before bed | Screens off or in warm/night mode; quiet, dim wind-down |
| Sleep | Bedroom as dark as possible — blackout curtains or eye mask |
A few notes on using the table well. First, the exact clock times do not matter — what matters is the order and the contrast: bright early, dim late, dark for sleep. Build it around your own wake time. Second, if you slip up (a bright late night out, a dim gray week indoors), just return to the pattern the next day; the clock is forgiving of occasional exceptions and responsive to consistent routine. Third, the single highest-leverage line in the table for most people is the first one — getting genuine daylight soon after waking — because it is free, low-risk, and supported by the most consistent evidence.
If your schedule is unusual (shift work, frequent travel across time zones), the same principles apply but the timing of bright versus dim light should be tailored to your target sleep window — a sleep clinician can help you plan this. Shift workers in particular need a customized strategy, because the goal may be to deliberately delay the clock rather than advance it, and generic “morning sun” advice can work against you if your “morning” is the afternoon.
Who should avoid this or proceed with caution
Light is generally safe, but it is not risk-free for everyone, and the cautions below matter especially if you are considering a bright light box or a red/near-infrared therapy device.
- Photosensitive conditions. People with conditions such as lupus or certain porphyrias, or other light-triggered disorders, should consult a doctor before increasing light exposure or using therapy devices.
- Photosensitizing medications. Some antibiotics, retinoids, certain psychiatric and acne medications, and others increase light sensitivity. Check with your pharmacist or physician.
- Eye and retinal conditions. If you have eye disease, recent eye surgery, or a retinal condition, get medical advice before bright-light therapy, and always follow eye-safety guidance and use eye protection with red/NIR devices, which can be intensely bright.
- Diagnosed sleep disorders. Insomnia, sleep apnea, and circadian rhythm sleep–wake disorders need proper evaluation. Light timing can be a powerful tool within a treatment plan, but self-treating a disorder can backfire.
- Mood disorders. In bipolar disorder, the timing of bright light can affect mood states; coordinate any light-therapy plan with your mental-health provider.
- Pregnancy. Talk to your provider before starting any new therapy device.
When in doubt, the safest move is to lean on the free, low-risk habits first — morning daylight and a dim evening — and bring any device-based plan to a qualified clinician. For authoritative, non-commercial background, see the Sleep Foundation’s guidance on light and sleep, the NIH National Institute of General Medical Sciences circadian rhythms page, and the Mayo Clinic overview of light therapy.
Conclusion
Better sleep through light is mostly about when and how bright, not about any single device. Front-load your day with real daylight, protect your evening melatonin by dimming and warming your light, and keep your bedroom dark. Red and near-infrared therapy has a small but legitimate place in that picture — chiefly because it is gentler on melatonin than blue-white light — but the direct evidence for red light improving sleep is still limited, and we will keep saying so until better data arrives.
If you want a device built for clinical-grade red and near-infrared output, with the controls to fit it into an evening wind-down responsibly, explore the RoyalPRO Series or browse everything in the shop. And whatever you try, anchor it to the habit that the science most consistently supports: bright mornings, dim nights.
- Your sleep is governed by a circadian rhythm — an internal ~24-hour clock that the brain sets primarily using light hitting the eye.
- Bright light in the morning anchors the clock and supports earlier, deeper sleep; bright light in the evening pushes the clock later and suppresses melatonin, the hormone that signals 'night' to the body.
- Ordinary indoor room light at night can cut melatonin by more than 50% and delay its release, according to a controlled Harvard study.
- Evidence that red or near-infrared light therapy directly improves sleep is limited and emerging — one small 14-day trial in athletes is the most-cited study, not proof for the general population.
- Red light's relevance to sleep is mainly that, unlike blue-rich light, it appears far less likely to suppress melatonin — so it is a gentler choice for evening use, not a sleeping pill.
- Photosensitive conditions, certain medications, and diagnosed sleep disorders all warrant a doctor's input before changing your light routine.
FREQUENTLY ASKED
Does red light therapy actually improve sleep?
The honest answer is: the evidence is limited and early. The most-cited study is a small 14-day trial in 20 elite female basketball players (Zhao et al., 2012) that reported improved sleep scores and higher melatonin. That is a promising signal, not proof for the general population. Far stronger and more consistent evidence supports the indirect route: getting bright light in the morning and avoiding bright, blue-rich light at night to keep your circadian clock and melatonin on schedule.
Is red light better than blue light before bed?
For protecting melatonin, yes — red and near-infrared wavelengths appear far less likely to suppress melatonin than blue-rich white light at the same brightness. A 2019 study found saturated red light delivered at low levels through closed eyelids did not suppress melatonin. So a warm, dim, red-leaning environment at night is a reasonable circadian-friendly choice. That is different from claiming red light is a treatment for insomnia.
When should I get morning light, and how much?
Aim to get outside within an hour or two of waking, ideally for 10–30 minutes. Outdoor daylight — even on an overcast day — is dramatically brighter than indoor lighting (thousands to tens of thousands of lux outdoors versus a few hundred indoors), and that brightness is what anchors your clock. You do not need to stare at the sun; ambient daylight reaching your eyes is enough.
How late at night does light affect sleep?
Light in the few hours before your usual bedtime is the most disruptive window, because that is when melatonin is normally rising. A controlled study found that room light before bedtime delayed melatonin onset and shortened its duration by roughly 90 minutes. Dimming lights and reducing screen brightness in the last 2–3 hours before bed is the practical takeaway.
Can I use a red light therapy device at night?
Many people use red/near-infrared panels in the evening, and the wavelength itself is unlikely to suppress melatonin the way bright blue-white light does. However, devices can be intensely bright, generate heat, and require eye protection; an over-stimulating session right before bed may be activating for some people. Treat it as part of a wind-down routine earlier in the evening rather than a lights-out ritual, and follow the device's eye-safety guidance.
Who should be cautious with light-timing changes?
Anyone with a photosensitive condition (such as lupus or certain forms of porphyria), anyone taking photosensitizing medication, people with eye disease or retinal conditions, and anyone with a diagnosed sleep disorder (insomnia, sleep apnea, a circadian rhythm disorder, or bipolar disorder, where light timing can affect mood) should talk to a qualified clinician before making changes.
REFERENCES
- 1. Blume C, Garbazza C, Spitschan M. Effects of light on human circadian rhythms, sleep and mood. Somnologie. 2019;23(3):147–156. PMC6751071
- 2. Tähkämö L, Partonen T, Pesonen A-K. Systematic review of light exposure impact on human circadian rhythm. Chronobiol Int. 2019;36(2):151–170. doi:10.1080/07420528.2018.1527773
- 3. Wright KP Jr, McHill AW, Birks BR, Griffin BR, Rusterholz T, Chinoy ED. Entrainment of the human circadian clock to the natural light-dark cycle. Curr Biol. 2013;23(16):1554–1558. PMC4020279
- 4. Boubekri M, Cheung IN, Reid KJ, Wang CH, Zee PC. Impact of windows and daylight exposure on overall health and sleep quality of office workers: a case-control pilot study. J Clin Sleep Med. 2014;10(6):603–611. doi:10.5664/jcsm.3780
- 5. Gooley JJ, Chamberlain K, Smith KA, et al. Exposure to room light before bedtime suppresses melatonin onset and shortens melatonin duration in humans. J Clin Endocrinol Metab. 2011;96(3):E463–E472. PMC3047226
- 6. Chang A-M, Aeschbach D, Duffy JF, Czeisler CA. Evening use of light-emitting eReaders negatively affects sleep, circadian timing, and next-morning alertness. Proc Natl Acad Sci USA. 2015;112(4):1232–1237. doi:10.1073/pnas.1418490112
- 7. Wams EJ, Woelders T, Marring I, et al. Linking light exposure and subsequent sleep: a field polysomnography study in humans. Sleep. 2017;40(12):zsx165. PMC5806586
- 8. Zhao J, Tian Y, Nie J, Xu J, Liu D. Red light and the sleep quality and endurance performance of Chinese female basketball players. J Athl Train. 2012;47(6):673–678. PMC3499892
- 9. Figueiro MG, Sahin L, Roohan C, Kalsher M, Plitnick B, Rea MS. Effects of red light on sleep inertia. Nat Sci Sleep. 2019;11:45–57. PMC6506010
ABOUT THE AUTHORS
Our team reviews the peer-reviewed literature on red and near-infrared light therapy and translates it into honest, practical guidance — no hype, just what the evidence actually supports.