Why 850 nm Penetrates Deeper Than 660 nm: Red Light Wavelengths and Tissue Depth
Why 850 nm near-infrared reaches deeper into tissue than 660 nm red light: tissue optics, the therapeutic window, absorption, scattering, and depths per wavelength.
If you compare two red light panels and one emits 660 nm while the other emits 850 nm, the 850 nm light reaches deeper into your body. The short answer to why is two-fold: longer near-infrared wavelengths are scattered less by skin and tissue, and they sit in a spectral region where your two biggest light-absorbers, hemoglobin in blood and melanin in skin, soak up comparatively little energy. Together, scattering and absorption decide how far light travels, and 850 nm wins on both counts compared with visible red.
But “deeper” is measured in millimeters, not the centimeters that marketing sometimes implies. This article walks through the actual tissue optics: the optical window, what absorbs and scatters light in skin, where 660 nm versus 850 nm each do their work, approximate depths with sources, why good devices combine both, and how to choose a wavelength by goal. The numbers come from peer-reviewed measurements, and we flag honestly where the science is uncertain.
First, a few definitions used throughout. Wavelength is the length of one light wave, measured in nanometers (nm) — one nanometer is a billionth of a meter. Irradiance (also called power density) is how much light power lands on a given area, usually milliwatts per square centimeter (mW/cm²). Absorption is when a molecule captures a photon and converts its energy (into heat or a chemical change). Scattering is when light changes direction without being absorbed — the dominant reason light spreads out and loses its way in tissue.
The optical window: where tissue lets light through
Living tissue is not transparent, but it is not uniformly opaque either. There is a band of wavelengths — roughly 600 to 1100 nm — where skin and soft tissue are at their most see-through. Scientists call this the optical window or therapeutic window, and it exists because the substances that absorb light most strongly happen to leave a gap there.
On the short-wavelength side (below ~600 nm, i.e. blue, green, yellow, and the start of red), hemoglobin and melanin absorb light heavily. On the long-wavelength side (above ~1100 nm), water — which makes up most of your tissue — begins to absorb strongly. In between, neither chromophore dominates, so a larger fraction of light survives to travel deeper.
Both wavelengths used in red light therapy live inside this window. Reviews of photobiomodulation describe the practical therapeutic range as approximately 600 nm to 1100 nm, with shorter wavelengths used for superficial tissue and longer wavelengths used for deeper-seated targets (Avci et al., 2013; Hamblin, 2016). The foundational measurements behind this picture go back to Anderson and Parrish, whose 1981 study mapped how human skin transmits, reflects, and absorbs light across the spectrum (Anderson & Parrish, 1981).
Why 660 nm and 850 nm both sit inside it
- 660 nm (deep red) is near the long edge of visible light, just inside the window. Hemoglobin absorption has fallen off considerably from its peaks in the green/yellow, so red light already travels meaningfully better than, say, blue.
- 850 nm (near-infrared, NIR) sits comfortably in the middle of the window, past the visible range entirely. It avoids most of what little hemoglobin and melanin absorption remains at 660 nm, and it is still well below the wavelengths where water absorption ramps up.
That position is the core reason 850 nm out-penetrates 660 nm: it is simply in a quieter part of the spectrum where less light is taken out of the beam per millimeter traveled.
What absorbs and scatters light inside skin
To understand depth, you have to track two competing fates for every photon: it can be absorbed (captured and converted) or scattered (bounced off course). Penetration depth is whatever is left after both processes chip away at the beam.
The main absorbers (chromophores)
- Melanin — the pigment in the epidermis. It absorbs strongly in the ultraviolet and visible range and tapers off into the near-infrared. More melanin (darker or more tanned skin) means more absorption near the surface, which reduces how much visible red light gets past the epidermis. This is one reason individual results and effective dose can differ with skin tone.
- Hemoglobin (oxygenated and deoxygenated) — in blood. It has strong absorption peaks in the visible region (notably in the green/yellow and into red) that drop off by the near-infrared. This is why blood-rich tissue blocks shorter wavelengths more than 850 nm.
- Water — the bulk of tissue. It is fairly transparent across the optical window but becomes a major absorber beyond ~1100 nm, which sets the long-wavelength edge of the window.
Detailed spectra for skin, fat, and mucosa across 400–2000 nm were measured by Bashkatov et al. (2005), and they show exactly this layout: a relatively low-absorption corridor through the red and near-infrared, flanked by hemoglobin/melanin below and water above.
Scattering: the bigger obstacle for deep light
In most soft tissue, scattering matters more than absorption within the optical window. Tissue is full of microscopic structures — cell membranes, collagen fibers, organelles — with refractive-index differences that deflect light. A photon entering your skin typically scatters many times before it is finally absorbed or exits.
The key fact for our question: scattering decreases as wavelength increases. Longer wavelengths are deflected less by these microscopic structures, so they keep moving forward instead of being diffused sideways and back out of the skin. That is why 850 nm, with its longer wavelength, holds a more directional, deeper-reaching path than 660 nm even where their absorption is similar. Reduced scattering at longer wavelengths is a consistent finding across tissue-optics measurements (Bashkatov et al., 2005).
So the deeper reach of 850 nm comes from two effects pulling the same direction:
- Less absorption — it sits in a low-hemoglobin, low-melanin part of the window.
- Less scattering — longer wavelengths are deflected less by tissue microstructure.
Red 660 nm vs NIR 850 nm: where each one acts
It helps to think of the two wavelengths as having different “addresses” in your tissue.
660 nm — the skin specialist
Visible red light is largely a surface and shallow-dermis wavelength. It is strongly absorbed by the upper layers, so it deposits most of its energy in the epidermis and papillary dermis — exactly where skin-focused goals live (collagen-producing fibroblasts sit in the dermis). Computational modeling shows red light penetrating notably better than blue but still being mostly attenuated within the first few millimeters: in Monte Carlo simulations, blue light barely cleared 1 mm while red extended to roughly 4–5 mm before falling to 1% of incident intensity (Ash et al., 2017). Because much of 660 nm energy is absorbed shallow, it is efficient for the skin and wasteful for anything deep.
850 nm — reaching toward muscle and joint
Near-infrared at 850 nm carries a larger surviving fraction into the deeper dermis and subcutaneous tissue, putting it in better range of muscle, tendon, and joint targets. The clearest direct demonstration of the red-versus-NIR difference comes from cadaver work: Jagdeo et al. (2012) measured light transmission through human cadaver tissue and found that near-infrared (830 nm) measurably penetrated soft tissue, bone, and brain, while red light transmission was essentially negligible through the same structures. The amount that got through still varied dramatically by location — for example, transmission of 830 nm light through the skull ranged from under 1% at the temporal region to about 11.7% at the occipital region — underscoring that even NIR is heavily attenuated.
Approximate penetration depths (with sources)
There is no single correct depth number, and any device that gives you a precise one without qualification is overselling. “Penetration depth” varies with the tissue, the pigmentation and blood content, the irradiance, and even how you define the cutoff (often the depth at which intensity falls to 1/e — about 37% — or to 1% of the surface value). With that caveat, here is an honest synthesis of the measured literature.
| Wavelength band | Approximate effective reach in skin/soft tissue | Best-for tissue target |
|---|---|---|
| Blue/green (~450–550 nm) | Sub-millimeter; largely stopped within ~1 mm | Very superficial epidermis (not used in red light panels) |
| Red 630–660 nm | Most energy deposited within ~1–3 mm; modeling shows ~4–5 mm to the 1% level | Epidermis and dermis: skin surface, visible appearance |
| Near-infrared 800–850 nm | Larger surviving fraction into the deeper dermis/subcutis; still strongly attenuated within a few mm | Deeper dermis, subcutaneous tissue, toward muscle/joint |
| ~1000–1100 nm | Near the deep edge of the window before water absorption rises | Deepest tissue targets, limited by rising water absorption |
The sobering reality checks come from real measurements. Transmission of 820 nm light drops to roughly 10% through 2 mm of skin and becomes essentially undetectable by 3 mm, as reviewed by Henderson (2024), who measured only a few percent of near-infrared energy surviving through skull samples and a fraction of a percent through a 2.5 cm hand. The takeaway is not that light therapy fails — it is that the usable depth is a few millimeters of soft tissue, and dose at the target matters far more than headline depth claims. The simulation work in Ash et al. (2017) and the optical-property tables in Bashkatov et al. (2005) point the same way: deeper than red, but still measured in millimeters.
Penetration is not the same as benefit
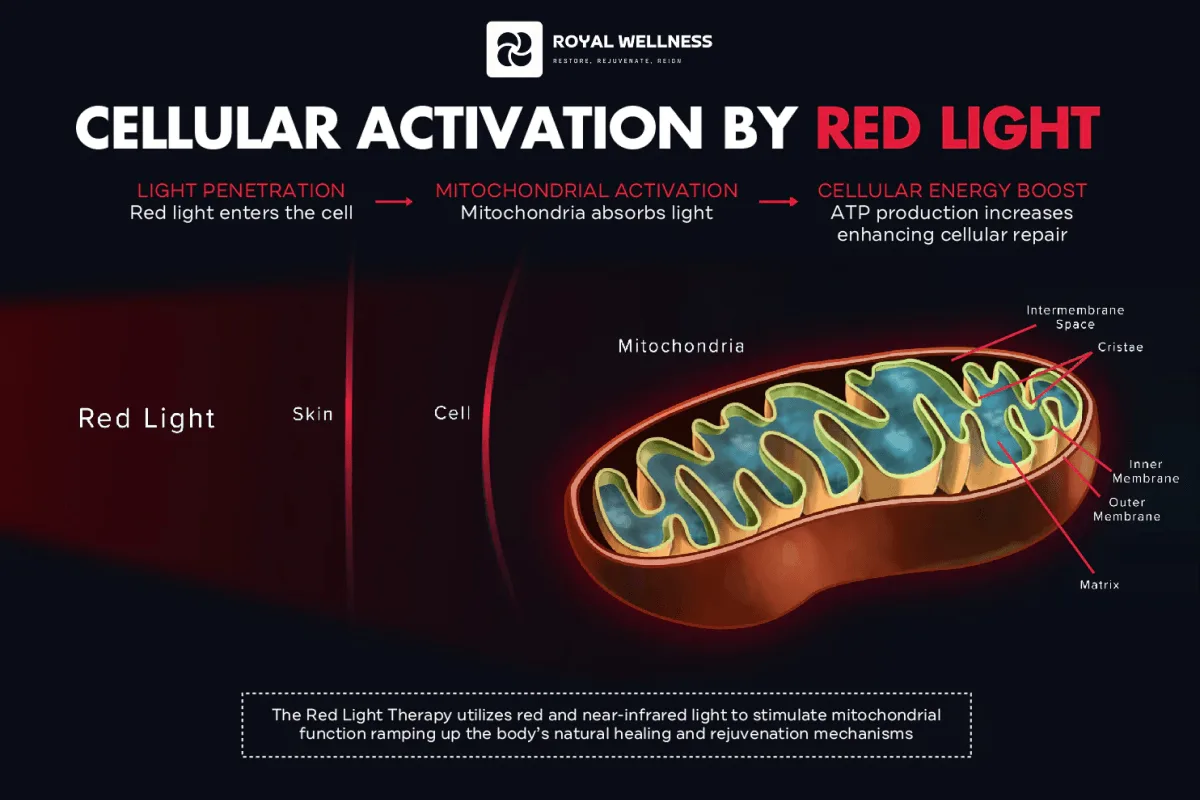
This is the most important honest framing in the whole topic. Light arriving at a depth is necessary for an effect there, but not sufficient. The light still has to be absorbed by the right chromophore — in photobiomodulation, primarily cytochrome c oxidase in the mitochondria — and deliver an effective dose. The proposed mechanism is that red/NIR photons are absorbed by this enzyme, increasing ATP production and triggering downstream signaling (de Freitas & Hamblin, 2016). Crucially, dose follows a biphasic response: too little does nothing, and too much can suppress the effect (Zein et al., 2018). So a wavelength that penetrates well but is dosed poorly can underperform a shallower wavelength dosed correctly. Penetration buys you access, not a guaranteed result.
Why good devices combine 660 nm and 850 nm
If 660 nm is a skin specialist and 850 nm reaches deeper, the obvious move is to use both — and that is precisely what well-designed panels do. The two wavelengths cover complementary depth ranges in a single session:
- 660 nm delivers more energy where the skin’s fibroblasts and surface tissue are, supporting skin-focused goals.
- 850 nm carries usable energy further toward muscle, connective tissue, and joints.
The dermatology literature on LED therapy reflects this dual-wavelength logic: light-emitting diodes are used across the red and near-infrared range precisely because different depths and targets call for different wavelengths (Barolet, 2008). Combining them is not a marketing gimmick; it is a direct consequence of tissue optics — no single wavelength is optimal for both surface and depth.
You can read more about how we think about device design on the science page, and browse the underlying studies in our research library.
Choosing wavelengths by your goal
Use the depth logic in reverse: start from where your target tissue is, then pick the wavelength that reaches it efficiently.
- Skin surface and appearance (epidermis, shallow dermis): favor 630–660 nm. The energy lands where you want it instead of passing through.
- Deeper soft tissue (muscle, tendon, joints near the surface): favor 850 nm, which retains more energy at depth.
- Both at once: a combined 660 nm + 850 nm device covers shallow and deeper targets in one session — the most common practical choice.
A few practical reminders that the optics imply:
- Distance and time set the dose. Irradiance falls off with distance, so being too far away can drop the dose below the effective range regardless of wavelength. Follow the manufacturer’s recommended distance and duration.
- Skin tone affects surface absorption. More melanin absorbs more visible red near the surface; this is a real variable in how much light reaches the dermis, not a defect.
- More is not better. Because the dose response is biphasic, longer or closer is not automatically more effective (Zein et al., 2018).
A brief safety note on invisible light
There is one safety point specific to 850 nm that does not apply to visible red. Near-infrared light is invisible, so your eyes do not respond to it with the blink or aversion reflex they use to protect against bright visible light. That means you can over-expose your eyes to NIR without any sensation warning you to look away.
The practical rule is simple: use the eye protection provided with your device, do not stare directly into the emitters, and follow the manufacturer’s distance and exposure guidance. Red and near-infrared light at therapeutic levels is non-ionizing and generally well tolerated, but the invisibility of 850 nm makes eye protection the one habit worth being strict about.
The bottom line
850 nm penetrates deeper than 630–660 nm for two reinforcing reasons rooted in tissue optics: it scatters less because it is a longer wavelength, and it is absorbed less because it sits in a quiet stretch of the optical window between hemoglobin/melanin and water. Real measurements — computational (Ash et al., 2017), cadaveric (Jagdeo et al., 2012), and optical-property tables (Bashkatov et al., 2005) — confirm the direction while keeping us honest about scale: the difference plays out over millimeters, and most light is absorbed or scattered within a few millimeters of soft tissue. Penetration is the entry ticket, not the show; an effective dose at the target tissue is what actually drives the proposed biological effects.
That is why the smartest approach is rarely “one wavelength.” Matching 660 nm to surface and skin goals and 850 nm to deeper tissue — ideally in a single combined device — lets the optics work for you instead of against you.
Want a device engineered around both wavelengths with disclosed irradiance and clear distance guidance? Explore the RoyalPRO Series, dig into the evidence in our research library, or shop the full range. For the deeper mechanism background, see the science.
- 850 nm near-infrared penetrates deeper than 630–660 nm red light mainly because longer wavelengths are scattered less by tissue and sit in a region where blood and melanin absorb less light.
- The 'optical window' (roughly 600–1100 nm) is the band where tissue is most transparent: above it water absorption rises sharply, below it hemoglobin and melanin absorb strongly.
- Red light (630–660 nm) does most of its work at the skin surface and shallow dermis; 850 nm reaches further toward subcutaneous tissue, with measurable transmission falling off within a few millimeters of tissue.
- Penetration is not the same as clinical benefit. Real cadaver and computational measurements show most light is absorbed or scattered within millimeters, so dose at the target tissue matters more than marketing depth claims.
- Devices combine 660 nm and 850 nm to cover both shallow (skin) and deeper (muscle, joint) targets in one session.
- 850 nm is invisible. Because the eye cannot trigger a blink or aversion reflex to near-infrared, eye protection is the key safety consideration for NIR devices.
FREQUENTLY ASKED
Does 850 nm really penetrate deeper than 660 nm?
Yes, but modestly and over millimeters, not centimeters. Longer near-infrared wavelengths scatter less in tissue and fall in a spectral band where blood and melanin absorb less, so a larger fraction of 850 nm light reaches a given depth than 660 nm. Computational modeling (Ash et al., 2017) and cadaver transmission studies (Jagdeo et al., 2012) both show near-infrared reaching further than red, while still being heavily attenuated within a few millimeters.
How deep does each wavelength actually reach?
There is no single number, because 'penetration depth' depends on tissue type, pigmentation, blood content, and how you define it. As a rough guide from the literature, visible red light is largely attenuated within roughly the first 1–3 mm of skin, while 800–850 nm light retains a usable fraction a bit deeper into the dermis and subcutaneous layer. Even so, transmission of 820 nm light drops to about 10% through 2 mm of skin and is essentially undetectable by 3 mm (reviewed in Henderson, 2024).
What is the optical or therapeutic window?
It is the wavelength band, roughly 600–1100 nm, where skin and tissue are relatively transparent. Below ~600 nm, hemoglobin and melanin absorb light strongly; above ~1100 nm, water absorption rises sharply. Both 660 nm and 850 nm sit inside this window, which is why red and near-infrared are the wavelengths used in photobiomodulation (Avci et al., 2013; Hamblin, 2016).
If 850 nm goes deeper, why use 660 nm at all?
Because depth is only useful if the target is deep. Skin-surface goals such as the visible dermis and epidermis are well served by 630–660 nm, which deposits more of its energy where you want it. For muscle, tendon, or joint targets, 850 nm reaches further. Combining both covers shallow and deeper tissue, which is why many panels emit both wavelengths.
Does deeper penetration mean better results?
Not automatically. Penetration tells you light arrives; it does not guarantee a biological effect. The light still has to deliver an effective dose (irradiance times time) to the target chromophores, and both under-dosing and over-dosing reduce the response (Zein et al., 2018). Treat penetration as a necessary condition, not proof of benefit.
Is 850 nm light safe if I cannot see it?
The light itself is non-ionizing, but invisibility is exactly why eye protection matters. Your eyes cannot trigger a blink or aversion reflex to near-infrared the way they do to bright visible light, so you can over-expose the retina without discomfort. Use the eye protection supplied with your device and follow the manufacturer's distance and time guidance.
REFERENCES
- 1. Anderson RR, Parrish JA. The optics of human skin. J Invest Dermatol. 1981;77(1):13–19. anderson-parrish-1981
- 2. Ash C, Dubec M, Donne K, Bashford T. Effect of wavelength and beam width on penetration in light-tissue interaction using computational methods. Lasers Med Sci. 2017;32(8):1909–1918. doi:10.1007/s10103-017-2317-4 ash-2017
- 3. Bashkatov AN, Genina EA, Kochubey VI, Tuchin VV. Optical properties of human skin, subcutaneous and mucous tissues in the wavelength range from 400 to 2000 nm. J Phys D Appl Phys. 2005;38(15):2543–2555. doi:10.1088/0022-3727/38/15/004 bashkatov-2005
- 4. Avci P, Gupta A, Sadasivam M, et al. Low-level laser (light) therapy (LLLT) in skin: stimulating, healing, restoring. Semin Cutan Med Surg. 2013;32(1):41–52. avci-2013
- 5. Barolet D. Light-emitting diodes (LEDs) in dermatology. Semin Cutan Med Surg. 2008;27(4):227–238. doi:10.1016/j.sder.2008.08.003 barolet-2008
- 6. Hamblin MR. Shining light on the head: photobiomodulation for brain disorders. BBA Clin. 2016;6:113–124. doi:10.1016/j.bbacli.2016.09.002 hamblin-2016
- 7. de Freitas LF, Hamblin MR. Proposed mechanisms of photobiomodulation or low-level light therapy. IEEE J Sel Top Quantum Electron. 2016;22(3):348–364. doi:10.1109/JSTQE.2016.2561201 defreitas-hamblin-2016
- 8. Jagdeo JR, Adams LE, Brody NI, Siegel DM. Transcranial red and near infrared light transmission in a cadaveric model. PLoS One. 2012;7(10):e47460. doi:10.1371/journal.pone.0047460 jagdeo-2012
- 9. Zein R, Selting W, Hamblin MR. Review of light parameters and photobiomodulation efficacy: dive into complexity. J Biomed Opt. 2018;23(12):120901. doi:10.1117/1.JBO.23.12.120901 zein-2018
- 10. Henderson TA. Can infrared light really be doing what we claim it is doing? Infrared light penetration principles, practices, and limitations. Front Neurol. 2024;15:1398894. doi:10.3389/fneur.2024.1398894 henderson-2024
ABOUT THE AUTHORS
Our team reviews the peer-reviewed literature on red and near-infrared light therapy and translates it into honest, practical guidance — no hype, just what the evidence actually supports.