Red Light Therapy for Muscle Recovery: What the Science Actually Shows
How red and near-infrared light affects muscle recovery, DOMS, and performance — the mechanisms, dosing in J/cm², timing, and wavelengths that matter.

Does red light therapy help muscle recovery?
Yes — but with honest caveats. Across dozens of randomized controlled trials and several meta-analyses, red and near-infrared light (a method researchers call photobiomodulation, or PBM) has been shown to reduce delayed-onset muscle soreness, lower blood markers of muscle damage such as creatine kinase, and produce small improvements in how quickly strength returns after hard training. The signal is most consistent when the light is delivered before exercise rather than after [4][5][6].
The effects are real, but they are modest, not miraculous. Some well-run studies report no meaningful benefit, and one systematic review concluded that low-level phototherapy “may not have substantial effect” on exercise-induced muscle injury overall [7]. The most useful way to read the evidence: red light is a legitimate, low-risk tool that can nudge recovery in the right direction when the dose and timing are correct — not a replacement for sleep, protein, and smart programming. This article walks through the mechanism, what the trials actually found, how to dose it, which wavelengths matter, and who should be cautious.
A quick note on terminology, because the field uses several names for the same thing. You will see low-level laser therapy (LLLT), light-emitting diode therapy (LEDT), cold laser, and photobiomodulation (PBM) used interchangeably across the studies cited below. The underlying principle is identical — non-thermal red or near-infrared light absorbed by tissue to trigger a biological response. PBM is now the preferred scientific umbrella term, and it covers both laser and LED light sources. For home recovery, LED panels deliver the same wavelengths that the laser trials used, just spread over a larger area at lower power density.
The mechanism: light, mitochondria, and ATP
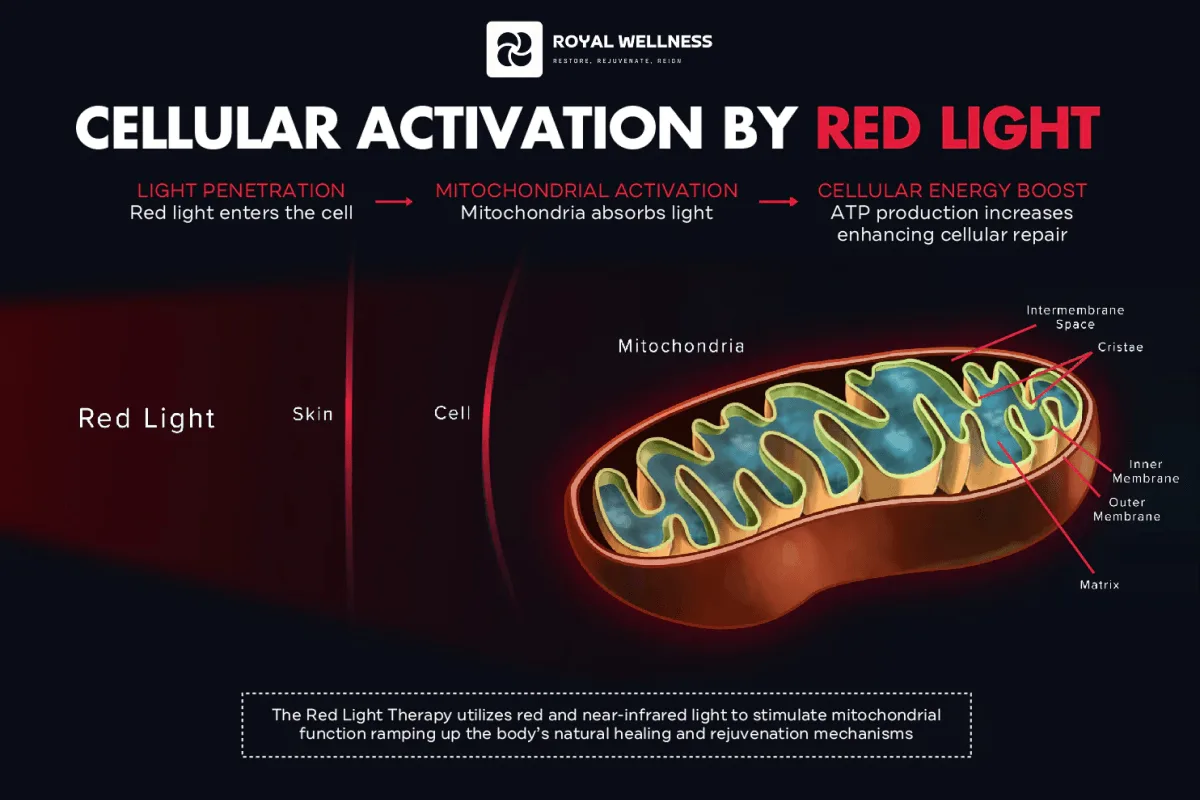
To understand why a wavelength of light could touch muscle recovery at all, you have to start inside the cell. Photobiomodulation is the use of red or near-infrared light at non-thermal doses to trigger biological responses in tissue — it works through a photochemical reaction, not by heating you up.
The primary target, or chromophore, is an enzyme in the mitochondria called cytochrome c oxidase. When red/near-infrared photons are absorbed there, they appear to displace inhibitory nitric oxide and improve the flow of electrons through the respiratory chain. The downstream result is more ATP — the cell’s energy currency — along with a brief, signaling burst of reactive oxygen species and changes in calcium handling [1].
Those first-order events ripple outward. In oxidatively stressed or inflamed tissue, PBM tends to lower overall oxidative stress and activate transcription factors — including NF-κB and others — that improve cell survival, proliferation, and repair [1]. In muscle specifically, this translates to better mitochondrial function and reduced markers of damage and inflammation after exertion [2][3].
Why does this matter for recovery? Intense exercise — especially the eccentric, lengthening contractions that drive soreness — temporarily impairs mitochondrial efficiency, floods the tissue with reactive oxygen species, and kicks off an inflammatory cascade. That cascade is part of normal adaptation, but when it is excessive or prolonged, it slows the return to full function. The proposed value of red light is that it helps the cell’s energy machinery recover faster and keeps oxidative and inflammatory signaling from overshooting [1][2]. In a treadmill-running trial, for example, pre-exercise light therapy measurably reduced post-exercise oxidative damage to both lipids and proteins compared with placebo, alongside lower creatine kinase and lactate dehydrogenase — direct biochemical evidence of the antioxidant effect playing out in human muscle [9].
Two features of muscle make it an especially good candidate for PBM. First, muscle is densely packed with mitochondria, so there is a large population of the exact chromophore the light targets. Second, near-infrared wavelengths penetrate well enough to reach those fibers (more on depth below). Together, that means a meaningful share of an effective dose can actually arrive where it is needed [2][3].
Why “biphasic dose” is the single most important idea
PBM follows a biphasic dose-response: a small amount of light stimulates, while too much can inhibit the very same processes [1]. This is why more is not better. Blasting tissue with excessive energy or sitting too close for too long can erase the benefit. Getting the dose into the effective “window” matters more than session length or perceived intensity.
What the evidence shows for DOMS, strength, and recovery
Let’s translate the lab biology into outcomes athletes actually care about.
Delayed-onset muscle soreness (DOMS)
DOMS is the dull ache and stiffness that peaks roughly 24 to 72 hours after unaccustomed or eccentric exercise, driven by microscopic damage to muscle fibers and the inflammatory response that follows (Cleveland Clinic). In a randomized, double-blind, placebo-controlled trial, a single LED phototherapy treatment at 630 nm applied immediately after damaging eccentric exercise meaningfully attenuated muscle soreness and reduced strength loss and range-of-motion impairment over the following days [10].
A dedicated meta-analysis on phototherapy and DOMS was more cautious: pooling 15 studies in 317 participants, it found that benefits were inconsistent across the literature, and that the clearest reduction in creatine kinase appeared specifically when light was applied before the exercise protocol [7]. The takeaway is nuanced — light can help with soreness, but pre-exercise timing is where the data is strongest. This is also a useful reminder that not every study is positive; a responsible reading of the evidence holds the encouraging trials and the null results in the same hand.
It helps to understand what creatine kinase (CK) actually tells you. CK is an enzyme that leaks into the bloodstream when muscle fibers are damaged, so a smaller post-exercise rise in CK is taken as a sign that less damage occurred — or that the tissue is coping better. Several trials report exactly that pattern with pre-exercise PBM [8][9][10]. CK is an indirect marker rather than a direct measure of how you feel, which is why the best studies pair it with subjective soreness scores, strength testing, and range-of-motion measures — and the LED trial above moved all of those in the right direction [10].
Strength, fatigue, and performance
A meta-analysis of 39 trials in healthy people found that PBM improved muscular performance and reduced exercise-associated fatigue, with positive effects clustered in the 655–950 nm range [6]. An earlier systematic review reached a similar conclusion: phototherapy administered before resistance exercise consistently provided “ergogenic and prophylactic benefits,” including delayed fatigue onset and improved recovery [4].
In a progressive-intensity treadmill study, low-level laser therapy applied before running significantly increased time to exhaustion and VO2 max while lowering post-exercise oxidative damage to lipids and proteins versus placebo [9]. And in a dose-finding trial, pre-exercise near-infrared laser at 810 nm improved performance and damage/inflammation markers — with a 50 J dose per site outperforming both 10 J and 30 J [8]. That single result captures the central practical lesson of this whole field: the dose that “works” is a specific number, and both too little and too much fall short of it.
It is worth being precise about what “performance” means here, because the gains are real but bounded. We are talking about a few extra repetitions before failure, a modestly longer time to exhaustion, slightly better strength retention across a damaging session, and lower fatigue — not transformation [4][6]. For a competitive athlete chasing marginal gains, even a small, reliable edge in recovery between sessions can compound over a training block. For a recreational lifter, the more tangible benefit is usually feeling less wrecked the day after a hard leg or pull session.
How to read these results honestly
- The most reliable benefit is pre-exercise (preconditioning), where multiple reviews converge [4][5][6].
- Post-exercise use can still reduce soreness and damage markers, but results are more variable [7][10].
- Effect sizes are generally small to moderate. Red light optimizes recovery; it does not override poor sleep, under-fueling, or excessive training load.
Dosing and timing: irradiance vs. dose
This is where most home users go wrong, so let’s define the two numbers that matter.
- Irradiance (mW/cm²) is the power density — how intensely the light hits the skin at a given moment. It is set by your device’s output and your distance from it.
- Dose (J/cm²) is the total energy delivered — irradiance multiplied by time. This is the number tied to outcomes in the research.
A simple way to remember it: irradiance is how hard the faucet runs; dose is how much water ends up in the bucket. Because of the biphasic curve, the goal is to land in the effective dose window — not to maximize either number.
The math connecting them is simple, and worth knowing so device marketing can’t mislead you. Dose in joules per square centimeter equals irradiance in milliwatts per square centimeter, multiplied by time in seconds, divided by 1,000. So a panel delivering 50 mW/cm² at your chosen distance reaches 6 J/cm² in two minutes (50 × 120 ÷ 1,000 = 6). Double the distance and irradiance falls off sharply — light obeys roughly an inverse-square relationship — so the same two minutes now delivers far less energy. This is exactly why a manufacturer’s tested distance-and-time chart matters more than a headline wattage number: total power means nothing without knowing how much of it actually lands on your skin and for how long.
There is also a difference between per-area dose (J/cm²) and total dose per muscle (J). The trials cited here tend to report total joules delivered to a muscle across multiple points, while panel users think in terms of J/cm² across an exposed surface. Both are valid; just don’t confuse a small per-point laser dose with the total energy a panel spreads across a whole muscle group.
A practical recovery protocol
The table below synthesizes dose ranges reported across the trials and reviews cited here [6][8]. Treat it as a starting framework, and always defer to the tested distance-and-time chart that ships with your specific device.
| Parameter | Small muscle group (e.g. biceps, forearm) | Large muscle group (e.g. quads, hamstrings, back) |
|---|---|---|
| Target dose | ~20–60 J total | ~60–300 J total |
| Wavelengths | 660 nm and/or 810–850 nm | 660 nm and/or 810–850 nm |
| Irradiance at skin | Comfortable, non-thermal (no burning sensation) | Comfortable, non-thermal |
| Typical session | A few minutes per area | A few minutes per area, covering the full muscle |
| Best timing | Before training (preconditioning) | Before training (preconditioning) |
| Frequency | Around training sessions; daily use is reasonable | Around training sessions; daily use is reasonable |
A few timing rules of thumb drawn from the evidence:
- Default to pre-exercise. Apply light to the muscles you’re about to load, 5–15 minutes before the session [4][8][9].
- Use post-exercise for soreness. If your priority is reducing next-day DOMS, a session immediately after the bout is supported [10].
- Don’t chase intensity. Once you hit the dose window, extra time offers diminishing — or even negative — returns [1].
You can go deeper on the underlying physics on our the science page and browse the studies behind these numbers in our research library.
Wavelengths: 660 nm vs. 810–850 nm
Not all “red light” reaches muscle. Penetration depth is governed largely by wavelength.
- 660 nm (visible red): Strongly absorbed in superficial tissue. Excellent for skin and the most superficial layers, and used successfully in DOMS trials [10], but it does not travel deep.
- 810–850 nm (near-infrared, NIR): Sits in the “optical window” where tissue absorbs and scatters less, so more of the light reaches deeper structures like muscle. Many of the strongest performance and recovery trials used NIR around 810–830 nm [8][9].
In practice, combining red and near-infrared is the common-sense approach for recovery: 660 nm covers superficial tissue and skin, while 850 nm carries energy toward the muscle belly. This is exactly why most serious recovery panels — including the RoyalPRO Series — emit both wavelengths rather than one. We cover the depth question in more detail in our wavelength explainer within the research library.
A couple of practical clarifications that come up constantly:
- Visible vs. invisible. Red light at 660 nm is bright and obviously “on.” Near-infrared at 850 nm is largely invisible to the human eye — you may see only a faint dim glow even when the diodes are at full output. A panel that looks dimmer is not necessarily weaker; it may simply be running more of its power in the near-infrared band you can’t see.
- Skin tone and tissue. Melanin and blood absorb red light more strongly than near-infrared, so on deeper muscle the NIR fraction does most of the meaningful work. Red wavelengths still earn their place for surface tissue, skin, and the soreness response.
- It is not about getting a tan or warmth. Penetration here is a photochemical phenomenon, not a thermal one. The light is reaching tissue and being absorbed by mitochondria whether or not you feel anything.
How to use red light for recovery at home
Turning the evidence into a routine is straightforward once the device is dialed in.
- Expose bare skin. Light has to reach the tissue; clothing and even thin fabric block a large fraction of the dose.
- Set the right distance. Follow your device’s tested chart. Closer means higher irradiance and a shorter time to reach the same dose; farther means lower irradiance and longer sessions.
- Time it to your training. For performance and damage prevention, treat the muscles you’re about to work before the session [4][8].
- Cover the whole muscle. Move a smaller device methodically, or use a full panel to treat large groups like quads and back in one pass.
- Keep it non-thermal. You should feel gentle warmth at most. Red light therapy is not a heat treatment — if your skin feels hot, you’re too close.
- Be consistent. Recovery benefits accumulate with a regular routine layered on top of good sleep, protein intake, and load management.
If you’re choosing hardware, our shop breaks devices down by coverage area and use case, and the RoyalPRO Series is built around dual 660/850 nm output for full-body recovery work.
Where red light fits in a real recovery routine
Red light is a multiplier, not a foundation. The biggest recovery levers remain unglamorous: enough sleep, adequate protein and total calories, hydration, and a training load your body can actually absorb. Photobiomodulation works best layered on top of those — and several studies deliberately tested it as an add-on, not a replacement [4][6].
A realistic weekly approach for most people:
- On training days, apply light to the target muscles before your session for the preconditioning effect, and consider a second pass after especially damaging work [4][8][10].
- On hard-volume or competition days, prioritize the muscles taking the most load — quads after a heavy squat day, posterior chain after deadlifts or sprints.
- On rest days, light use is reasonable and low-risk, though the clearest documented benefits are tied to exercise sessions [6].
Set expectations accordingly. If you sleep five hours and under-eat, red light will not rescue your recovery. If your fundamentals are solid, it is a credible way to shave the edge off soreness and return to training a little fresher. That is a worthwhile outcome — just not a substitute for the basics.
Who should avoid it
Red and near-infrared light has a strong safety profile in healthy adults, but it is not for everyone. Talk to a qualified clinician before use — and in some cases avoid it entirely — if any of the following apply:
- Active cancer over the treatment site. Because PBM stimulates cellular activity, do not treat directly over a known or suspected malignancy without oncology guidance.
- Pregnancy. Avoid treating over the abdomen and seek medical clearance before broader use.
- Photosensitizing medication or conditions. Some drugs (certain antibiotics, retinoids, St. John’s wort, and others) and conditions increase light sensitivity and can cause adverse skin reactions.
- Eye exposure. Near-infrared light is invisible but can still reach the retina. Use the eye protection your device specifies and never stare into the source.
The bottom line
Red light therapy for muscle recovery is one of the better-studied applications of photobiomodulation, and the evidence is genuinely encouraging: reduced soreness, lower muscle-damage markers, less oxidative stress, and small but real improvements in recovery and performance — most reliably when light is applied before you train [4][5][6][8]. The mechanism is sound (mitochondrial absorption, more ATP, less inflammation), and the safety profile is excellent for healthy adults [1][2].
It is not magic, and the literature is honest about that — dose, timing, and wavelength all have to be right, and red light works best stacked on top of solid fundamentals. If you want a device engineered for recovery dosing with both 660 nm and 850 nm output, explore the RoyalPRO Series or compare full-body options in our shop.
- Across controlled trials and meta-analyses, red and near-infrared light (photobiomodulation) can reduce delayed-onset muscle soreness and creatine kinase while modestly improving recovery — the strongest, most consistent effect appears when light is applied BEFORE exercise.
- The mechanism is light absorption by cytochrome c oxidase in mitochondria, which raises ATP output, lowers oxidative stress, and dampens inflammation — not heat.
- Dose is what matters most: roughly 20–60 joules per small muscle group and 60–300 J for large groups (655–950 nm), delivered at a comfortable, non-thermal intensity.
- 660 nm (red) targets superficial tissue; 810–850 nm (near-infrared) penetrates deeper toward muscle — many recovery protocols combine both.
- Effects are real but modest, not magic; the literature also includes null results, so treat red light as one recovery tool alongside sleep, protein, and load management.
- Avoid use over active cancers, during pregnancy without clearance, and if you take photosensitizing medication; always protect the eyes from direct near-infrared output.
FREQUENTLY ASKED
Does red light therapy actually help muscle recovery?
Yes, the modality has measurable effects. Multiple randomized trials and meta-analyses report reduced delayed-onset muscle soreness, lower creatine kinase (a muscle-damage marker), and small improvements in strength recovery after photobiomodulation, especially when light is applied before exercise. The effects are consistent but modest, and some studies show no benefit, so it is best viewed as a supportive tool rather than a cure-all.
Should I use red light before or after a workout?
The strongest evidence is for pre-exercise application. Reviews of low-level laser and LED therapy found that 'preconditioning' muscles with light before training most reliably delayed fatigue and reduced post-exercise damage markers. Post-exercise use can still help with soreness, but if you have to choose one window, the research favors before.
What wavelength is best for muscle recovery — 660 nm or 850 nm?
Both have value because they reach different depths. Red light around 660 nm is absorbed in superficial tissue, while near-infrared at roughly 810–850 nm penetrates deeper toward muscle. Many positive trials used near-infrared (around 810–830 nm) or a red-plus-near-infrared combination, which is why most recovery panels offer both.
How long should a muscle recovery session be?
Long enough to deliver an effective dose without overheating the skin — often a few minutes per area at a comfortable distance. What matters is the total energy (joules) reaching the tissue, roughly 20–60 J for a small muscle group and 60–300 J for a large one, not the clock. Follow your device's tested distance-and-time chart.
Is red light therapy safe for muscle recovery?
For healthy adults, non-thermal red and near-infrared light has a strong safety profile in the research literature, with few serious adverse effects reported. Caution is warranted over active cancers, during pregnancy without medical clearance, and with photosensitizing medication, and you should always shield your eyes from direct near-infrared light.
Can red light therapy replace rest, sleep, or protein?
No. Red light may speed how quickly muscles bounce back, but the foundations of recovery are still sleep, adequate protein, hydration, and sensible training load. Think of photobiomodulation as a way to optimize an already-solid recovery routine, not a substitute for it.
REFERENCES
- 1. Hamblin MR. Mechanisms and applications of the anti-inflammatory effects of photobiomodulation. AIMS Biophys. 2017;4(3):337–361. doi:10.3934/biophy.2017.3.337
- 2. Ferraresi C, Huang YY, Hamblin MR. Photobiomodulation in human muscle tissue: an advantage in sports performance? J Biophotonics. 2016;9(11–12):1273–1299. doi:10.1002/jbio.201600176
- 3. Ferraresi C, Hamblin MR, Parizotto NA. Low-level laser (light) therapy (LLLT) on muscle tissue: performance, fatigue and repair benefited by the power of light. Photonics Lasers Med. 2012;1(4):267–286. doi:10.1515/plm-2012-0032
- 4. Borsa PA, Larkin KA, True JM. Does phototherapy enhance skeletal muscle contractile function and postexercise recovery? A systematic review. J Athl Train. 2013;48(1):57–67. doi:10.4085/1062-6050-48.1.12
- 5. Leal-Junior EC, Vanin AA, Miranda EF, de Carvalho PT, Dal Corso S, Bjordal JM. Effect of phototherapy (low-level laser therapy and light-emitting diode therapy) on exercise performance and markers of exercise recovery: a systematic review with meta-analysis. Lasers Med Sci. 2015;30(2):925–939. doi:10.1007/s10103-013-1465-4
- 6. Vanin AA, Verhagen E, Barboza SD, Costa LOP, Leal-Junior ECP. Photobiomodulation therapy for the improvement of muscular performance and reduction of muscular fatigue associated with exercise in healthy people: a systematic review and meta-analysis. Lasers Med Sci. 2018;33(1):181–214. doi:10.1007/s10103-017-2368-6
- 7. Nampo FK, Cavalheri V, Ramos SP, Camargo EA. Effect of low-level phototherapy on delayed onset muscle soreness: a systematic review and meta-analysis. Lasers Med Sci. 2016;31(1):165–177. doi:10.1007/s10103-015-1832-4
- 8. Vanin AA, De Marchi T, Tomazoni SS, et al. Pre-exercise infrared low-level laser therapy (810 nm) in skeletal muscle performance and postexercise recovery in humans: what is the optimal dose? A randomized, double-blind, placebo-controlled trial. Photomed Laser Surg. 2016;34(10):473–482. doi:10.1089/pho.2015.3992
- 9. De Marchi T, Leal Junior ECP, Bortoli C, Tomazoni SS, Lopes-Martins RAB, Salvador M. Low-level laser therapy (LLLT) in human progressive-intensity running: effects on exercise performance, skeletal muscle status, and oxidative stress. Lasers Med Sci. 2012;27(1):231–236. doi:10.1007/s10103-011-0955-5
- 10. Borges LS, Cezar AF, Kuipers M, et al. Light-emitting diode phototherapy improves muscle recovery after a damaging exercise. Lasers Med Sci. 2014;29(3):1139–1144. doi:10.1007/s10103-013-1486-z
- 11. Cleveland Clinic. Delayed Onset Muscle Soreness (DOMS): What It Is & Treatment. Cleveland Clinic Health Library. Cleveland Clinic Health Library
ABOUT THE AUTHORS
Our team reviews the peer-reviewed literature on red and near-infrared light therapy and translates it into honest, practical guidance — no hype, just what the evidence actually supports.