Red Light Therapy for Collagen and Wrinkles: What Realistic Anti-Aging Results Actually Look Like
Does red light therapy boost collagen and smooth wrinkles? Here is what controlled trials show, the wavelengths that matter, and realistic 8-12 week results.

Short answer: Yes, red light therapy can boost collagen, and the evidence for it is better than most cosmetic claims. In controlled trials, red and near-infrared light increased the skin’s intradermal collagen density and measurably reduced wrinkles, fine lines, and roughness compared with untreated skin. But realistic results are gradual and modest: think smoother texture, slightly firmer skin, and softer fine lines over 8 to 12 weeks of consistent use, not a dramatic overnight transformation. This article walks through how it works on collagen, the wavelengths that actually matter, what the trials found, and what you can honestly expect.
Red light therapy, more precisely called photobiomodulation (PBM), uses specific wavelengths of red and near-infrared light to nudge cells toward better function. It is not a heat treatment and not UV, so it does not tan or burn skin the way a sunbed does. For anti-aging, the goal is straightforward: stimulate the fibroblasts in your dermis to rebuild collagen and elastin, the proteins that keep skin firm and smooth. If you want the deeper biology, our the science page covers photobiomodulation in detail, and our research library collects the studies referenced here.
How red light therapy works on collagen
Collagen is the structural protein that makes up most of your dermis. As you age, two things happen at once: your fibroblasts make less new collagen, and enzymes called matrix metalloproteinases (MMPs), especially MMP-1, break down more of the collagen you already have. The result is thinner, less elastic skin, with fine lines and wrinkles. Anything that shifts that balance, more collagen synthesis and less breakdown, can slow or partly reverse visible aging.
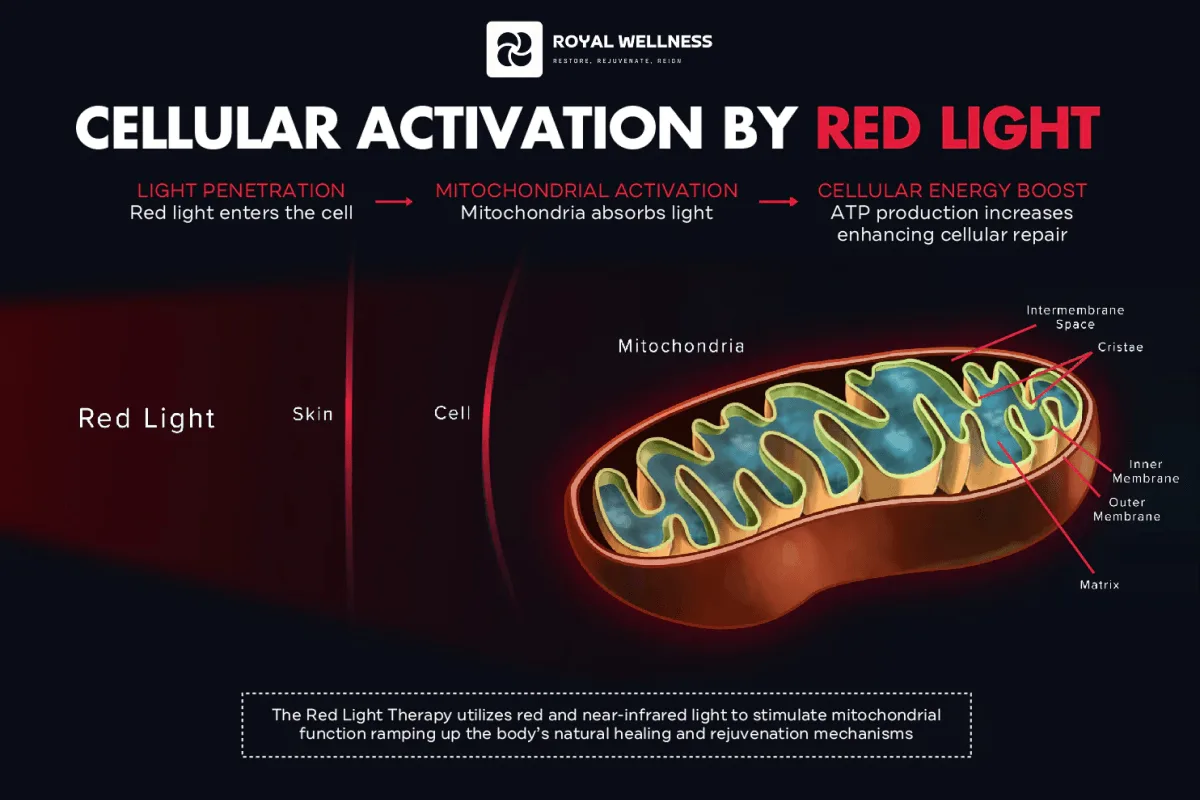
The mechanism: light into cellular energy
Photobiomodulation works at the level of the mitochondria, the energy factories inside your cells. The leading explanation is that red and near-infrared photons are absorbed by an enzyme called cytochrome c oxidase, a key component of the mitochondrial electron transport chain. When this enzyme absorbs light in the right wavelength range, it works more efficiently, producing more ATP (adenosine triphosphate, the cell’s energy currency), a brief, signaling-level burst of reactive oxygen species, and the release of nitric oxide. Michael Hamblin’s widely cited mechanism review describes this cascade as the foundation of how PBM influences cell behavior (Hamblin, 2017).
For skin, the downstream effect is what counts: energized fibroblasts become more active. Fibroblasts are the dermal cells responsible for manufacturing collagen, elastin, and the rest of the extracellular matrix that gives skin its structure. When their mitochondria run more efficiently, they have more energy available to synthesize these proteins, and gene-expression studies show that PBM can shift fibroblasts toward a more youthful, “build” state rather than a “break-down” state.
Laboratory and clinical work shows that the right light dose can increase type I procollagen (the precursor to new collagen) while reducing MMP-1. In a tissue-engineered human skin model paired with a clinical study, Barolet and colleagues reported a roughly 31% increase in type I procollagen and an 18% decrease in MMP-1 in light-treated skin compared with untreated skin, and most participants showed reduced wrinkle depth and roughness after a course of treatments (Barolet et al., 2009). Because this study measured both the biochemistry (procollagen and MMP-1) and the visible outcome (wrinkle depth) in the same project, it is a useful bridge between “what happens in cells” and “what shows up in the mirror.”
Why “more is not always better”
One quirk of photobiomodulation is the biphasic dose response. A moderate, appropriate dose of light stimulates cells; too little does nothing, and too much can actually inhibit the response. This is why dose (intensity and time) and wavelength matter so much, and why blasting your skin for an hour will not give you better results than a sensible session. The Avci review of LLLT in skin lays out this dose-dependence and the broad range of skin applications, from rejuvenation to wound healing (Avci et al., 2013).
The wavelengths that matter for skin
Light is not interchangeable. The wavelength (measured in nanometers, nm) determines both which chromophores absorb it and how deep into tissue it travels. For skin and collagen, the research clusters tightly around two bands.
- Visible red light (around 630-660 nm). This is the classic “red light” you can see. It is well absorbed in the epidermis and upper-to-mid dermis, which is exactly where collagen-producing fibroblasts live. Wavelengths near 633 nm and 660 nm dominate the skin-rejuvenation literature.
- Near-infrared light (NIR, around 830-850 nm). This light is invisible and penetrates deeper than red. It is often combined with red for a broader effect, and 830 nm in particular has strong clinical support for skin.
Wavelengths much shorter than this (blue light, around 415 nm) are used for acne, not collagen, because they barely penetrate and target bacteria instead. Wavelengths in the so-called “optical window” of roughly 600-1000 nm are favored for tissue effects because melanin and water absorb them less, letting more light reach the dermis (Sorbellini et al., 2018).
Wavelength, depth, and skin benefit
The table below summarizes how the main skin-relevant wavelengths behave. Penetration depths are approximate and vary with skin tone, hydration, and device power.
| Wavelength | Type | Approx. skin depth | Primary relevance to anti-aging |
|---|---|---|---|
| ~415 nm | Visible blue | Very shallow (epidermis) | Targets acne bacteria, not collagen |
| ~630-633 nm | Visible red | Upper-to-mid dermis | Fibroblast stimulation, collagen synthesis |
| ~660 nm | Visible red | Mid dermis | Collagen synthesis, reduced MMP-1 |
| ~830 nm | Near-infrared | Deeper dermis | Collagen, elasticity, often combined with red |
| ~850 nm | Near-infrared | Deeper dermis/subcutis | Deeper tissue support, frequently paired with red |
The practical takeaway: a device that delivers validated red (around 630-660 nm), or a combination of red and near-infrared (around 830-850 nm), is what the skin-rejuvenation evidence actually supports. A 2024 comprehensive review of photobiomodulation on the skin reaches the same general conclusion, identifying red and NIR as the workhorse wavelengths for collagen, elasticity, and rejuvenation outcomes (Hernandez-Bule et al., 2024).
What controlled trials actually show
This is the part that separates marketing from medicine. Here is what the better-designed human studies found, and the important caveats.
Collagen density and wrinkles: the Wunsch & Matuschka RCT
The most-cited clinical evidence is a prospective, randomized, controlled trial of 136 volunteers. Participants were treated with red light (around 611-650 nm) or a broader red-plus-near-infrared spectrum (around 570-850 nm), roughly twice weekly over about 15 weeks (about 30 sessions), and compared with untreated controls. The treated groups showed statistically significant improvements in skin complexion, skin roughness (measured objectively by profilometry), and intradermal collagen density (measured by ultrasound), along with reduced fine lines and wrinkles (Wunsch & Matuschka, 2014). Notably, the broadband spectrum offered no clear advantage over red-only, reinforcing that the red band is doing much of the work. The combination of objective instruments (profilometry for roughness, ultrasound for collagen) and a no-treatment control group is what makes this trial stand out: the results are not just based on subjective self-report or before-and-after photos that lighting can flatter.
Wrinkles and elasticity: the Lee split-face study
In a prospective, randomized, double-blind, split-face study, 76 people with facial wrinkles were treated twice weekly for four weeks with 830 nm alone, 633 nm alone, a combination of both, or a sham light. The treatment groups showed objective reductions in wrinkles (up to 36%) and increases in skin elasticity (up to 19%) versus baseline, and biopsies showed increased collagen and elastic fibers (Lee et al., 2007). This is one of the cleaner demonstrations that the histology (more collagen) tracks with the visible result (fewer wrinkles).
At-home masks: the Couturaud red-LED study
For people considering a face mask specifically, a 2023 study followed volunteers using a red LED mask (around 630 nm) twice weekly for three months. The researchers reported reductions in crow’s feet wrinkle depth, increases in dermal density and elasticity, and lower roughness, with benefits persisting for several weeks after the sessions ended (Couturaud et al., 2023). This is a smaller study without a placebo arm, so weigh it accordingly, but it is directly relevant to the mask format.
Periocular wrinkles: a focused RCT
The delicate skin around the eyes is a common concern. A randomized controlled trial focused on the periocular area reported a roughly 30% reduction in periocular wrinkle volume with photobiomodulation, again with good tolerability (Mota et al., 2023).
Honest framing of the evidence
A few caveats are essential for reading this literature well:
- Studies vary in quality. The strongest evidence (Wunsch & Matuschka, Lee) is randomized and controlled; others are small, single-arm, or industry-linked. Treat the modality as supported, not every individual marketing claim as proven.
- Devices are not standardized. Wavelength, power density, dose, and treatment frequency differ across studies and products, so results from one device do not automatically transfer to another.
- Effect sizes are modest. Percent improvements in wrinkles and elasticity are real and measurable, but they describe gradual refinement, not the dramatic change of surgery or injectables.
- The evidence supports the modality, not specific outcome promises for any one product. Red light therapy is a wellness modality with encouraging clinical data; it is not a medical treatment for a disease.
Realistic expectations and timeline
Here is the honest version. Red light therapy is a slow, cumulative habit, not a quick fix. Collagen is built over weeks to months, so the timeline below reflects what trials and clinical experience suggest, assuming consistent use of a validated device.
| Timeframe | What is realistic to notice |
|---|---|
| Week 1-2 | Little to no visible change; some people report skin feels smoother or looks brighter |
| Week 3-6 | Early softening of fine lines, more even tone and texture for consistent users |
| Week 8-12 | The window where most controlled trials measured meaningful change in wrinkles, roughness, and firmness |
| Week 12+ | Continued, gradual improvement; benefits plateau and then require ongoing maintenance |
To set expectations honestly:
- Consistency beats intensity. The trials that worked used regular sessions (often two to five times per week) over 8 to 15 weeks. Sporadic use will not reproduce those results.
- Results are maintained, not permanent. Because collagen turns over continuously, stopping entirely will let gains fade over months. Most people keep a maintenance schedule.
- It pairs well with basics. Sun protection, not smoking, and a sensible skincare routine do the heavy lifting of prevention; red light is a complement, not a replacement.
- Individual variation is real. Age, baseline skin condition, skin tone, hormonal status, and how diligently you stick to the schedule all influence how much you notice. Two people on the same device can have meaningfully different results, which is one reason single before-and-after photos online are a poor guide to what you personally should expect.
How to use it at home: mask vs panel
Both masks and panels deliver the same therapeutic wavelengths; the difference is form factor, coverage, and dose.
Face masks
A mask sits directly against the face and follows its contours, so the light reaches the cheeks, around the eyes, the forehead, and the nasolabial area evenly with no aiming required. That conformity and convenience is why masks are popular for facial anti-aging specifically, and why the Couturaud study used a mask format. Masks tend to be lower-powered than large panels, which means shorter sessions but a stronger emphasis on doing them consistently over a longer program. For a purpose-built facial device, see the RoyalGLOW Mask.
Panels
Panels are larger, higher-powered units mounted on a stand or wall. They cover more of the body (useful if you also want red light for recovery or larger skin areas) and can deliver a higher dose per session, but they require you to position your face at the correct distance and stay still. They are a better fit if you want flexibility for full-body use as well as the face.
Getting the dose right
Whichever format you choose, the fundamentals are the same:
- Validated wavelengths. Look for devices specifying red (around 630-660 nm) and/or near-infrared (around 830-850 nm).
- Clean, bare skin. Remove makeup and heavy SPF first; some mineral sunscreens and pigments can block or scatter light.
- Follow the device program. More time is not better thanks to the biphasic dose response; follow the recommended session length and frequency.
- Be patient and consistent. Track progress with the same lighting and angle photos every few weeks rather than judging day to day.
You can compare device types on our shop page if you are deciding between a mask and a panel.
Who should avoid it (or check with a doctor first)
Red and near-infrared light therapy is well tolerated for most healthy adults, and trials consistently report few or no adverse effects. It is non-UV, so it does not carry the DNA-damage and skin-cancer risk of tanning. Still, some people should be cautious or seek medical clearance first:
- Pregnancy. There is limited safety data for red light therapy during pregnancy. Talk to your provider before use.
- Photosensitizing medications. Some drugs make skin more reactive to light, including certain antibiotics (tetracyclines, fluoroquinolones), some diuretics, certain antidepressants and antipsychotics, and oral acne medication such as isotretinoin. If you take a medication labeled for photosensitivity, get clearance first.
- Prescription retinoids on the treated skin. Retinoids (tretinoin, and to a lesser degree some over-the-counter retinols) increase cell turnover and can thin and sensitize the stratum corneum, and retinoids themselves are associated with photosensitivity (Ferguson & Johnson, 1986). Many people apply retinoids at night and use light therapy separately; check with your dermatologist about timing and combining them on the same skin.
- Active melasma or pigment disorders. Because melasma can be triggered or worsened by light and heat, people with active melasma should be cautious and consult a dermatologist; the relationship between visible light and pigmentation is complex.
- Photosensitive conditions. Conditions such as lupus or porphyria, or a history of light-triggered rashes, warrant medical advice before starting.
- Eyes. Always use the eye protection supplied with your device, or keep your eyes closed, especially with bright facial masks. Do not stare into the LEDs.
If any of these apply to you, the safest path is a quick conversation with your doctor or dermatologist before you begin.
The bottom line
The evidence for red light therapy and collagen is genuinely encouraging: randomized controlled trials show increased intradermal collagen density and measurable reductions in wrinkles, fine lines, and roughness using visible red (around 630-660 nm) and near-infrared (around 830-850 nm) light. The mechanism, photobiomodulation driving more ATP and more fibroblast collagen synthesis while curbing MMP-1, is well described. What it is not is a miracle. Results are modest, gradual, and dependent on consistent use over 8 to 12 weeks and beyond, and they require maintenance to last.
If you want a convenient, face-focused way to put this evidence to work, a purpose-built device that conforms to your face and delivers validated wavelengths is the practical choice. Explore the RoyalGLOW Mask to start a consistent routine, and read the underlying studies in our research library so you can judge the evidence for yourself.
- In controlled trials, red and near-infrared light increased intradermal collagen density and measurably reduced wrinkles, roughness, and fine lines versus untreated skin.
- The wavelengths that matter for skin are visible red (around 630-660 nm) and near-infrared (around 830-850 nm); red is absorbed in the upper dermis where fibroblasts live, NIR reaches deeper.
- The mechanism is photobiomodulation: light absorbed by mitochondria boosts ATP and signals fibroblasts to make more collagen and less collagen-degrading enzyme (MMP-1).
- Realistic results take consistency: most trials ran 8-15 weeks of sessions 2-5 times per week before measuring meaningful change.
- Expect modest, gradual improvement in texture, firmness, and fine lines, not a facelift; effects build over months and require ongoing use to maintain.
- Skip or get medical clearance first if you are pregnant, take photosensitizing medication, use prescription retinoids on treated skin, or have active melasma, and always protect your eyes.
FREQUENTLY ASKED
Does red light therapy really increase collagen?
Controlled studies support it. In a randomized controlled trial by Wunsch and Matuschka (2014), people treated with red or red plus near-infrared light showed a statistically significant increase in intradermal collagen density measured by ultrasound, alongside reduced wrinkles and roughness, compared with untreated controls. The proposed mechanism is photobiomodulation: light absorbed by mitochondria raises cellular energy (ATP) and signals skin fibroblasts to produce more collagen.
How long before I see results from red light therapy for wrinkles?
Most clinical trials ran 8 to 15 weeks with sessions two to five times per week before measuring meaningful change. Expect the first subtle improvements in skin feel and brightness within a few weeks, with firmness and fine-line changes building over 8 to 12 weeks of consistent use. Results are gradual and require ongoing maintenance.
What wavelength is best for collagen and anti-aging?
The evidence clusters around visible red light (roughly 630-660 nm) and near-infrared (roughly 830-850 nm). Red light is well absorbed in the upper-to-mid dermis where collagen-producing fibroblasts sit, while near-infrared penetrates deeper. Several trials combined both, and the Lee (2007) study found combined 830 nm and 633 nm performed well for wrinkles and elasticity.
Are at-home red light masks as effective as professional panels?
They work on the same principle, but dose and coverage differ. Masks sit close to the face and conform to its contours, which is convenient for facial anti-aging; panels deliver higher power over a larger area. What matters most is using a device with validated wavelengths at an adequate dose, consistently. Home devices are generally lower-powered, so consistency and longer programs matter more.
Is red light therapy safe for skin?
For most healthy adults, red and near-infrared light therapy is well tolerated, and trials report few or no adverse effects. It uses non-UV wavelengths, so it does not carry the DNA-damage risk of tanning. However, you should use eye protection, and get medical clearance if you are pregnant, take photosensitizing medication, use prescription retinoids on the area, or have active melasma.
Will the results last if I stop using it?
Benefits are maintained with continued use. Some studies, including Couturaud (2023), found improvements persisted for several weeks after sessions stopped, suggesting real structural change. But collagen turnover is ongoing, so most people treat red light therapy as a maintenance habit rather than a one-time fix.
REFERENCES
- 1. Wunsch A, Matuschka K. A Controlled Trial to Determine the Efficacy of Red and Near-Infrared Light Treatment in Patient Satisfaction, Reduction of Fine Lines, Wrinkles, Skin Roughness, and Intradermal Collagen Density Increase. Photomed Laser Surg. 2014;32(2):93-100. doi:10.1089/pho.2013.3616 (PMC3926176)
- 2. Avci P, Gupta A, Sadasivam M, et al. Low-level laser (light) therapy (LLLT) in skin: stimulating, healing, restoring. Semin Cutan Med Surg. 2013;32(1):41-52. PMID:24049929 (PMC4126803)
- 3. Barolet D, Roberge CJ, Auger FA, Boucher A, Germain L. Regulation of skin collagen metabolism in vitro using a pulsed 660 nm LED light source: clinical correlation with a single-blinded study. J Invest Dermatol. 2009;129(12):2751-2759. doi:10.1038/jid.2009.186 (PMID:19587693)
- 4. Lee SY, Park KH, Choi JW, et al. A prospective, randomized, placebo-controlled, double-blinded, and split-face clinical study on LED phototherapy for skin rejuvenation. J Photochem Photobiol B. 2007;88(1):51-67. PMID:17566756
- 5. Couturaud V, Le Fur M, Pelletier M, Granotier F. Reverse skin aging signs by red light photobiomodulation. Skin Res Technol. 2023;29(7):e13391. doi:10.1111/srt.13391 (PMC10311288)
- 6. Mota LR, Duarte IDS, Galache TR, et al. Photobiomodulation Reduces Periocular Wrinkle Volume by 30%: A Randomized Controlled Trial. Photobiomodul Photomed Laser Surg. 2023;41(2):48-56. doi:10.1089/photob.2022.0114 (PMID:36780572)
- 7. Hamblin MR. Mechanisms and applications of the anti-inflammatory effects of photobiomodulation. AIMS Biophys. 2017;4(3):337-361. doi:10.3934/biophy.2017.3.337 (PMC5523874)
- 8. Hernandez-Bule ML, Naharro-Rodriguez J, Bacci S, Fernandez-Guarino M. Unlocking the Power of Light on the Skin: A Comprehensive Review on Photobiomodulation. Int J Mol Sci. 2024;25(8):4483. doi:10.3390/ijms25084483 (PMC11049838)
- 9. Sorbellini E, Rucco M, Rinaldi F. Photodynamic and photobiological effects of light-emitting diode (LED) therapy in dermatological disease: an update. Lasers Med Sci. 2018;33(7):1431-1439. doi:10.1007/s10103-018-2584-8 (PMID:30006754)
- 10. Ferguson J, Johnson BE. Photosensitivity due to retinoids: clinical and laboratory studies. Br J Dermatol. 1986;115(3):275-283. PMID:3530309
ABOUT THE AUTHORS
Our team reviews the peer-reviewed literature on red and near-infrared light therapy and translates it into honest, practical guidance — no hype, just what the evidence actually supports.